Back to Blog
The hidden revenue leak in healthcare: Intake and scheduling (and how AI solves it)
Learn how specialty providers and health systems can safely harness AI to standardize intake diagnostics and book the right appointments faster.
.webp)
10 min read

.svg)
.svg)
.svg)
TL;DR
- Most healthcare revenue loss happens before the visit – during intake and scheduling
- Manual scheduling workflows break at patient identification, data collection, provider matching, and booking
- AI can safely power faster scheduling and smoother intake that improves patient experiences and prevents revenue leakage
Most healthcare organizations think about revenue leakage after the visit: denied claims, coding and billing errors, missed charges and uncollected payments. But a significant share of that loss happens much earlier, during intake and scheduling.
It rarely comes from one dramatic failure. It comes from small, predictable breakdowns that repeat on every shift: a call with too many holds and transfers, a patient matched to the wrong provider, an out-of-network appointment, an incomplete or burdensome intake process. All of this leads to friction that creates poor experiences, patients getting care elsewhere, or not getting the care that they need at all.
This article breaks down where and why those breakdowns happen, what a structured fix actually looks like, and where AI accelerates the work versus where it creates new risk.
Demand is growing. The workflow hasn't kept pace.
There's a frustrating paradox happening inside specialty healthcare right now. Patient demand is growing. Referral volume is climbing. And yet revenue keeps slipping.
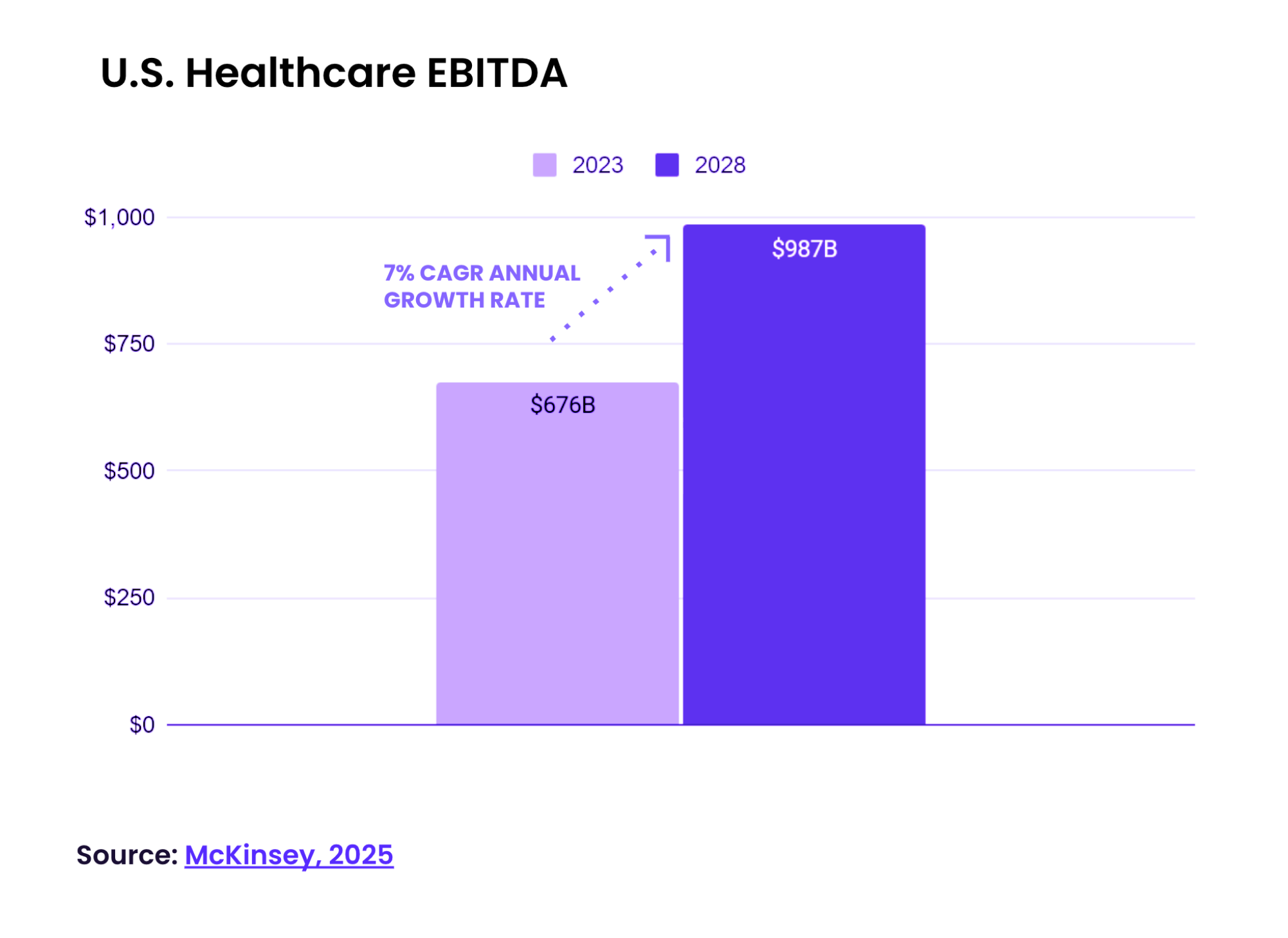
According to McKinsey's 2025 healthcare outlook, U.S. healthcare EBITDA is expected to grow at a 7% compound annual rate, reaching $987 billion by 2028.
But more volume doesn't automatically mean more revenue. It means more complexity: more specialties, more clinic locations, more payer rules, more support channels, and a staffing layer that hasn't scaled to absorb any of it.
When those conditions meet a fragmented intake workflow, every small inefficiency compounds into a significant financial problem.
The math is staggering:
- $150B annual cost of no-shows in the U.S.
- $5M average annual hospital loss from incomplete patient data
- $11.5M annual revenue loss from missed new patient acquisitions
Those are different problems on the surface. But they share the same pattern. Most of this leakage starts at first contact.
The problem isn't volume. It's what happens when a patient calls.
Ask any agent working a patient scheduling queue what their day looks like, and you'll hear a variation of the same story.
They're bouncing between screens: the EHR, the scheduling system, a spreadsheet, maybe a separate payer portal, trying to piece together who's calling and what they need before the patient gets frustrated and hangs up.
That's the first failure point: patient identification. And it leads directly to the second – provider matching, which is where the real complexity lives.
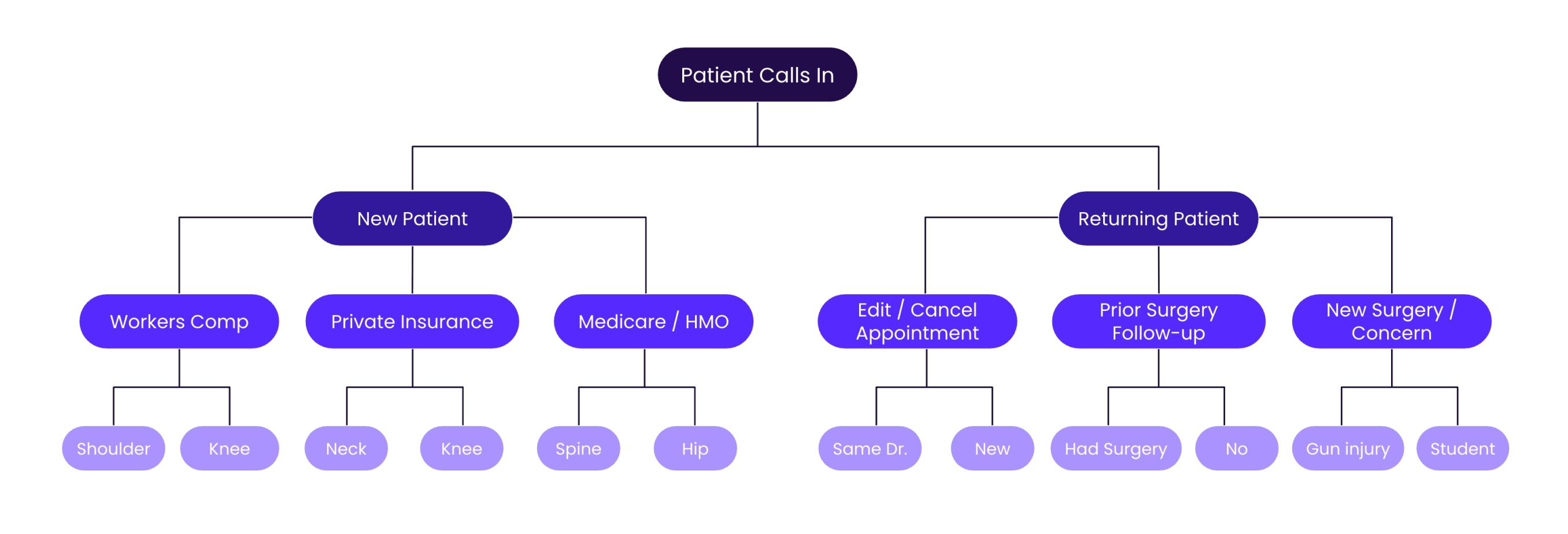
Consider what an agent at a large orthopedic practice actually has to figure out before booking an appointment:
- Is the patient covered under HMO, Medicare, or private insurance?
- Is the visit related to a workers' comp claim, a school injury, or something else entirely?
- What body part is affected, and does it require one provider or two?
- Has the patient had surgery before? Is this a first-time concern or a recurring one?
The operational drag runs deeper than most organizations track. Revenue leakage shows up across the entire front end: in eligibility denials driven by incomplete data collected at intake, in no-shows that follow incorrect provider matches, in scheduling gaps that go unfilled because calls weren't captured.
This is the everyday reality of specialty scheduling. And no human agent can hold all of it in their head reliably across every call.
Scheduling breaks in the same four places every time
Across different specialties and EHR environments, intake and scheduling failures tend to cluster around the same four moments in the call:
- ID breaks. The agent can't determine whether this is a new or returning patient without jumping systems. The patient ends up answering questions they've already answered. Context that should travel with the record disappears between calls.
- Data breaks. Coverage status, prior authorization, referral information – it all lives somewhere in the EHR or a separate payer portal, but it's not surfaced in the call. The agent is operating blind, making judgment calls they shouldn't have to make.
- Match breaks. Provider eligibility depends on combining multiple variables: coverage, concern, body area, visit history, prior surgery, location. Applying those rules manually is impossible without a structured decision layer.
- Book breaks. Even when the matching works, if no near-term slot is available, the patient goes elsewhere. And if the match was wrong, the appointment becomes a no-show.
Miss any one of these steps and the call turns into a revenue loss. Miss more than one, and it also becomes a compliance and patient safety risk: incomplete intake data leads to eligibility denials, incorrect routing creates clinical mismatch, and failure to document consent or HIPAA acknowledgments at intake creates downstream liability.
This is a permutations problem
Here's a concrete way to visualize why intake is so hard to standardize manually.
Take a mid-size orthopedic network: 30 offices, 200 clinicians, 20 payers, 300 distinct concerns, and 70 appointment slots per week per provider. The number of possible intake permutations is north of 2.5 billion.
No decision tree or static workflow can cover that. Certainly not at the speed patients expect. This is a textbook example of where AI takes CX automation to the next level: integrated into business workflows to scale, not break, under exponential complexity.
What actually happens in the absence of a structured decision layer is that agents default to what they know: the providers they recognize, the questions they remember, the paths they've taken before.
In specialty scheduling, this creates a specific secondary problem: provider utilization skews toward familiar names. A patient who calls about a shoulder gets booked with a provider the agent knows, while a clinician who is equally qualified and has more availability goes unbooked. At scale, across a network, this quietly distorts both revenue distribution and patient care quality in ways that never surface in aggregate dashboards.
The right response is embedding the logic in the workflow itself, so every agent follows the same path through the same decision tree, every time, regardless of how long they've been on the job.
What "standardized intake diagnostics" actually means
If intake breaks are predictable, the solution starts with standardization. The specific questions vary by specialty; mental health intake looks genuinely different from orthopedic triage. But the diagnostic categories are consistent across healthcare scheduling:
- Patient identification: new versus returning, and if returning, what was the prior interaction context?
- Insurance and coverage: what payer, what type of plan, any referral or prior authorization requirements?
- Reason for visit: what is the patient experiencing, and with what urgency?
- Clinical qualifiers: body area, injury history, prior surgery, any complicating factors that affect provider eligibility?
- Location and availability: geographic preference and how soon the patient needs to be seen?
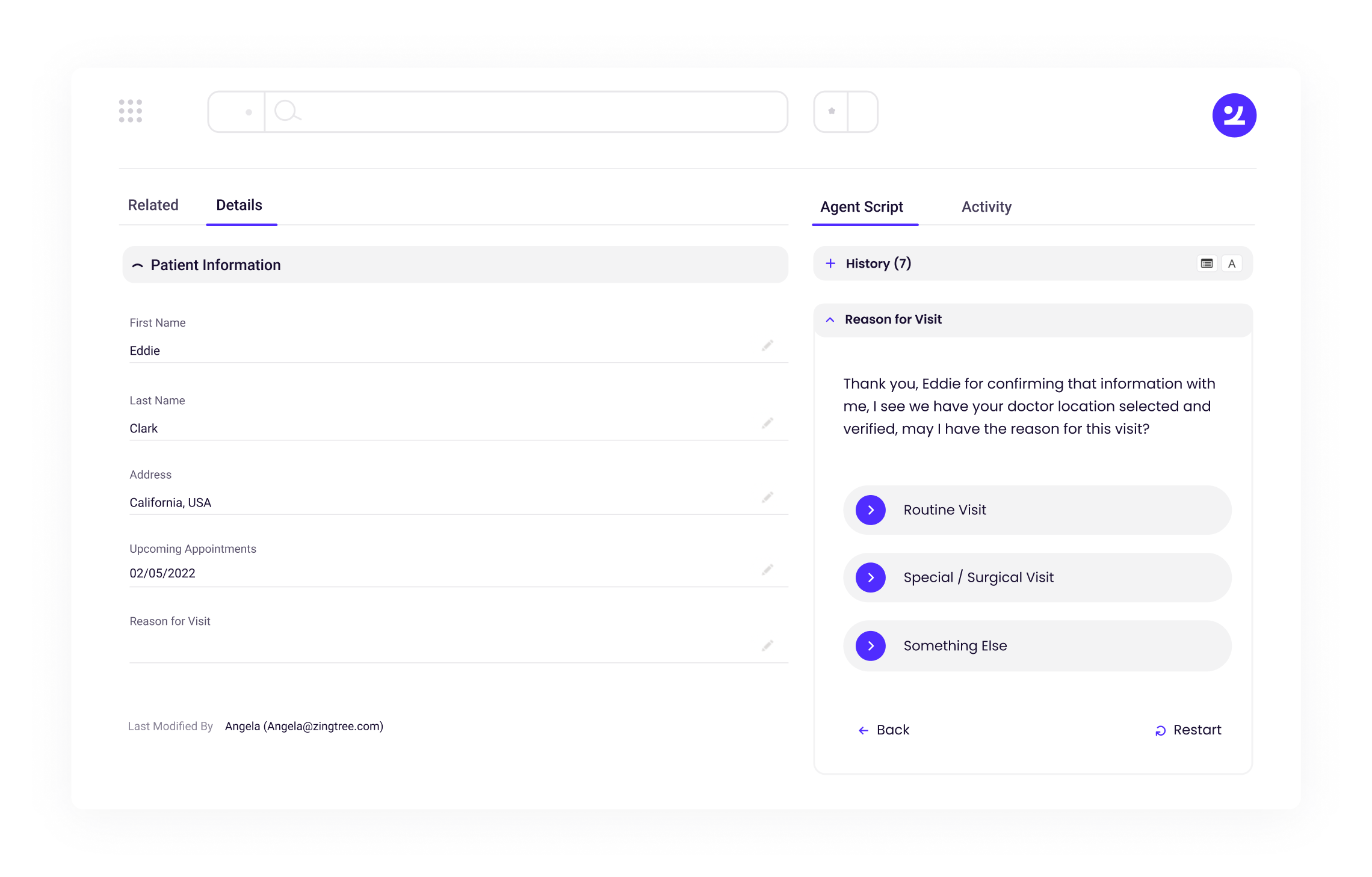
When these categories are embedded into a guided workflow, the number of variables an agent has to manage at once drops dramatically. The logic does the narrowing. The agent focuses on the conversation. The output is a shortlist of eligible, available providers rather than a best guess.
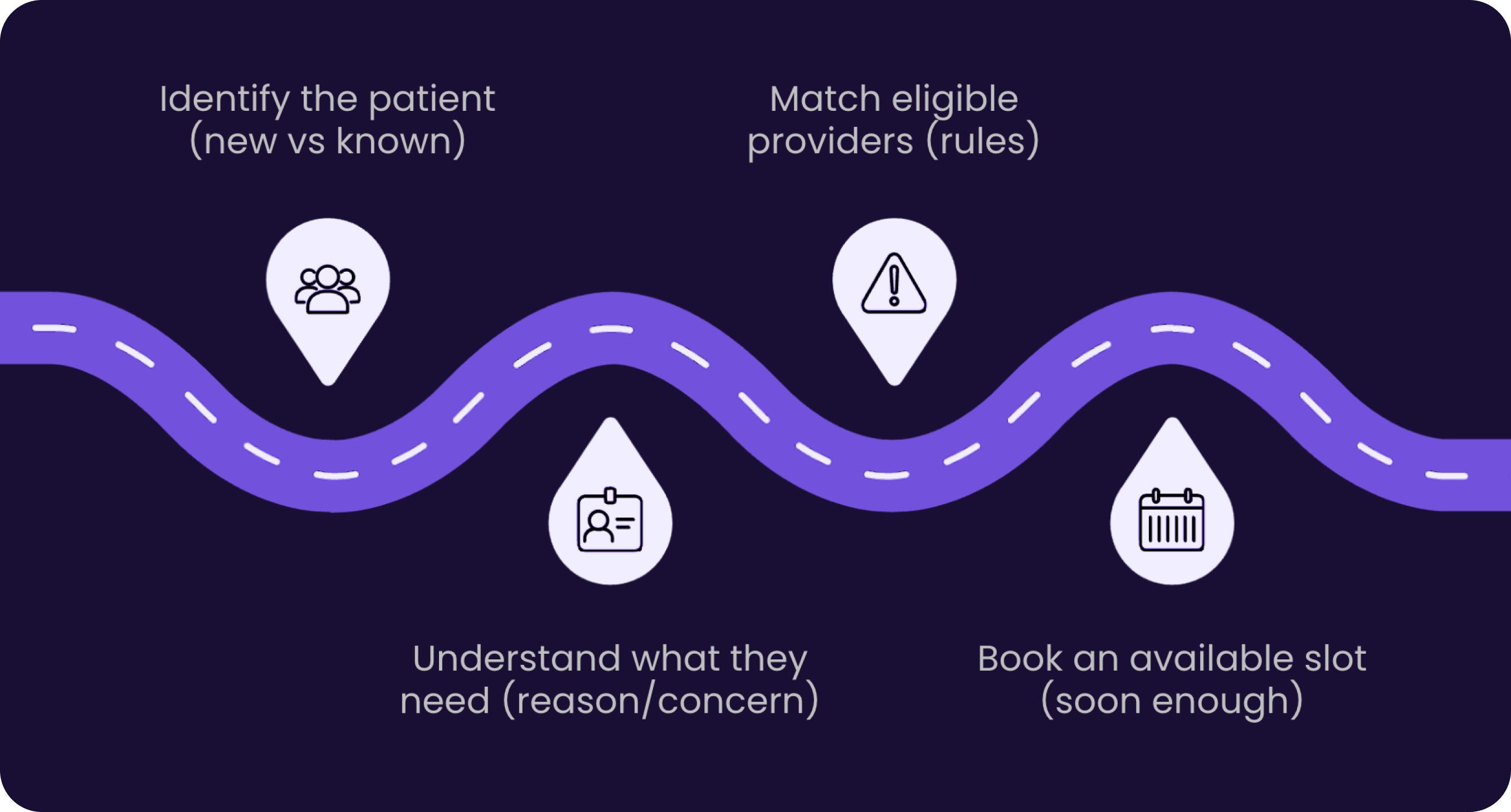
This is the standard diagnostic in motion: start with low context, narrow through three structured layers: identify the patient, determine visit type and urgency, confirm provider fit – and arrive at a bookable match. The flow replaces the swivel-chair work and the post-call copy-paste, because the system is capturing and routing in real time rather than after the fact.
When AI helps and when it creates new risks
AI has a meaningful role to play in scheduling and intake. But the organizations doing this well are deliberate about where they deploy it. The risk is that AI applied to a broken workflow accelerates the mistakes the workflow was already making.
If the data is scattered, incomplete, or inconsistently structured, AI produces unreliable outputs faster. Build the pipe first: a guided flow, usable data, explicit rules, and an audit trail. Then AI reduces steps safely.
Pre-call summarization is the clearest win. When a patient calls, AI can surface prior interaction history: why they called last time, what was scheduled, what changed, so the agent starts with context instead of cold. This alone removes several minutes of repetitive identification work from the front of every returning-patient call, and it reduces the number of repeated questions patients are asked across interactions.
Identity assist, matching an inbound phone number to the most likely patient record — reduces identification time and decreases the chance of starting a call with no context at all.
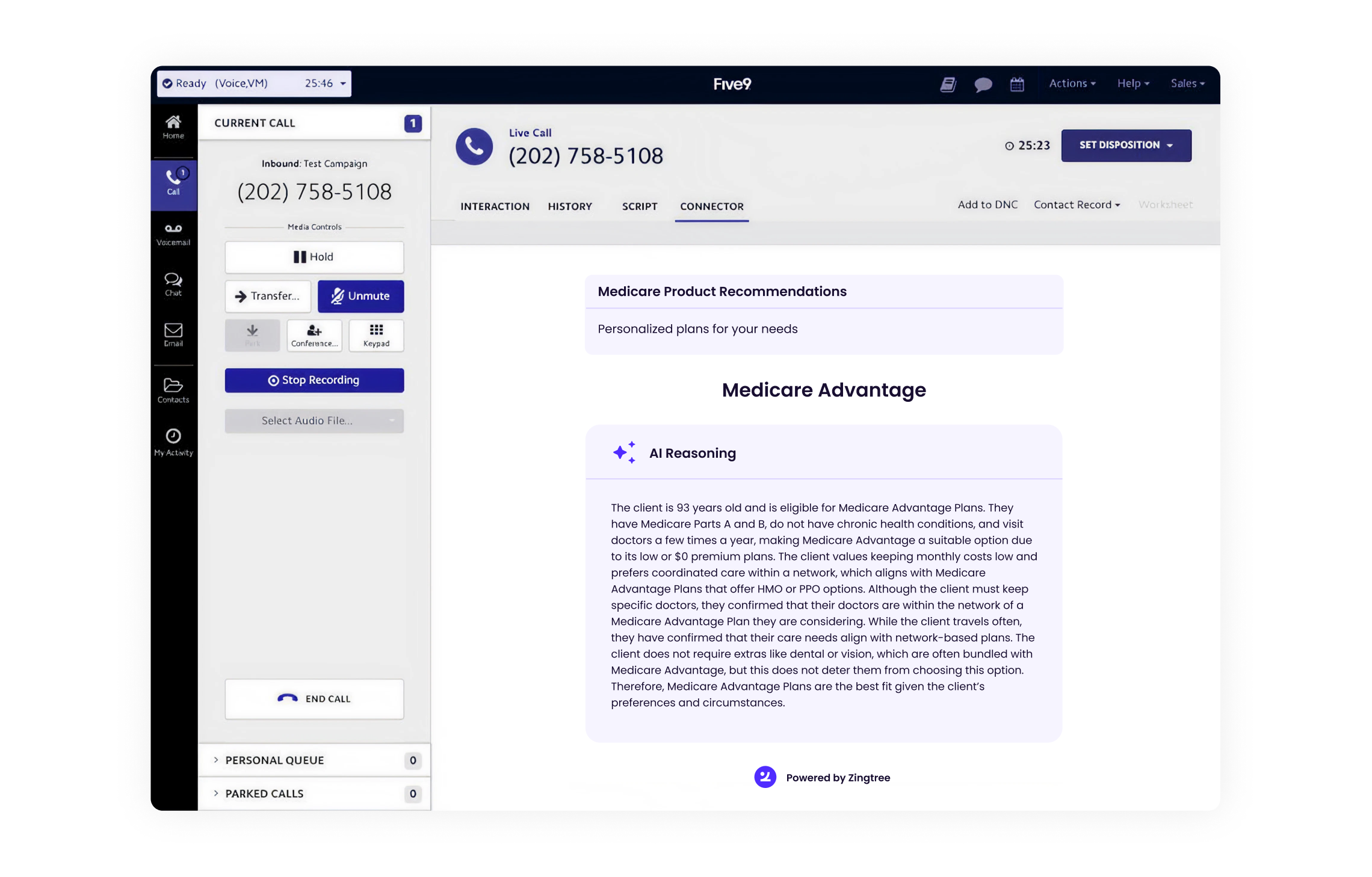
Provider matching assistance is a longer-term opportunity that replaces what currently requires complex conditional logic applied manually. The rules for matching a patient to an eligible provider — coverage type, concern, body area, visit and surgical history — are exactly the kind of multi-variable mapping that AI can handle reliably when the underlying data is structured and accessible.
Next-best action surfacing, displaying buttons that reflect logical next steps based on prior history and call context — removes the cognitive work of remembering what the next step is, especially for complex or unusual routing scenarios.
Where AI should not be the decision-maker: coverage verification without a confirmed source of truth, eligibility decisions that need to be explainable step-by-step for compliance purposes, and any booking action that must be auditable.
In regulated environments, the auditability requirement isn't optional. CMS and ONC interoperability rules increasingly require that patient data access and routing decisions be traceable — and that includes how automated systems arrive at scheduling recommendations.
What fixing intake looks like in practice
A large orthopedic network operating across multiple clinic locations faced a specific, measurable problem at the end of every scheduling call.
After agents completed the triage, matched the patient to a provider, and identified available slots, they had to manually copy and paste all captured data into the scheduling system. That process took approximately eight minutes per call — not because agents were slow, but because the systems weren't connected. Every agent did it slightly differently, and every copy-paste step introduced potential for error.
The intervention was a guided command center that standardized the qualifying questions, applied eligibility rules consistently across all agents, and used available API connections to write captured data back into the scheduling system directly. Post-call work dropped by roughly 85%. The estimated time savings: seven minutes per call, which translates into meaningfully more capacity per agent shift without adding headcount and a significant reduction in data errors that had been generating downstream rework in billing and coding.
What made the qualifying framework effective was its consistency. Four layers, applied the same way every time: coverage and insurance verification, reason for visit and urgency routing, clinical qualifiers affecting provider eligibility, and provider availability. Each layer narrowed the eligible provider set. The output was a shortlist plus available slots.
Ready to fix the front door?
The specialty practices making real progress on scheduling revenue leakage aren't starting with AI implementations or multi-year EHR integration projects. They're starting with the workflow: defining the minimum diagnostic categories their specialty requires, building a decision layer that applies those rules the same way every time, and solving the data accessibility problem well enough to support it.
If your team is still dealing with screen-jumping agents, post-call copy-paste, or inconsistent provider matching, those are solvable problems, and the fix is closer than it looks.
To learn more, we invite you to join us for a webinar with BerryDunn’s healthcare revenue cycle team on April 14th: Faster scheduling, smoother intake: How providers can safely use AI to improve patient experience.
Alternatively, you can reach out any time to talk to a Zingtree specialist about your scheduling workflow. We'll walk through where your intake process is leaking revenue and what a guided decision layer could look like for your specific specialty and EHR environment.
Frequently Asked Questions
What is healthcare revenue leakage in intake and scheduling?
Healthcare revenue leakage refers to lost revenue caused by breakdowns before the patient visit, including incorrect scheduling, incomplete intake data, and missed patient opportunities.
How does patient intake impact healthcare revenue?
Patient intake directly impacts revenue because missing or incorrect data can lead to eligibility denials, delays, and poor patient experiences that drive patients elsewhere.
Why is healthcare scheduling so complex?
Scheduling requires agents to evaluate multiple variables at once, including insurance type, referral status, clinical need, provider availability, and location. This complexity makes manual decision-making unreliable at scale.
How does AI improve healthcare intake and scheduling?
AI improves intake and scheduling by guiding agents through structured workflows, validating data in real time, and ensuring patients are matched to the right provider and appointment. It reduces errors and speeds up resolution.
What problems does AI solve in patient access workflows?
AI helps fix the four common failure points in patient access:
- Patient identification gaps
- Missing or incomplete data
- Incorrect provider matching
- Failed or delayed booking
These improvements lead to higher conversion, better patient experience, and reduced revenue leakage.
.png)

